آقای 78 ساله که با زخم نکروتیک انگشت بزرگ پای راست مراجعه نموده. سابقه نارسایی قلبی , CABG و دیابت را ذکر میکرده. وی به مدت سه ماه زیر نظر جراح عروق بوده ولی بهبودی در زخم حاصل نشده تا اینکه جهت درمان اندواسکولار به مرکز ا جعه نمود.
در معاینه بالینی نبض فمورال سالم بود اما نبض های پوپلیته و دیستال نداشت.
IN CATH LAB
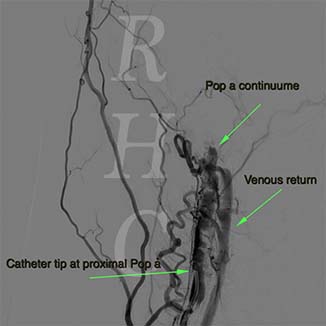
Diagnostic angiography using antegrade approach; the SFA was approached using US
This is a TASC D occlusion of Fem-Popliteal region. The trifurcation also is involved in these case retrograde approach also can be considered. Distal run off was acceptable and ATA which was visible at the trifurcation site can be seen with continuum DP. The other vessel which was seen at distal was PA, and because PTA was totally occluded PA and ATA patency became more crucial
 
Antegrade wiring was done by a stiff terumo wire and a regular A1 catheter. Checking the wire position is mandated during traverse through the occlusion. You see the path is Ok, and there is a shadow of immediate venous return; AVF also could be but as the wire and catheter is completely in artery lumen so this has lower probability. The right picture shows the distal part of occlusion. Wiring of ATA was impossible , as this is the case in such situations
 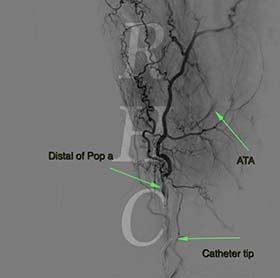 Retrograde access was achieved using US. As the ATA was a good vessel with good run off we choose that to cannulate. The problem was the only vessel supply the foot, ATA, might be damaged and change the situation elective into emergency. I prefer to use a 4 F glide catheter instead of sheath ion in order to lessen vessel damage.
Retrograde access was achieved using US. As the ATA was a good vessel with good run off we choose that to cannulate. The problem was the only vessel supply the foot, ATA, might be damaged and change the situation elective into emergency. I prefer to use a 4 F glide catheter instead of sheath ion in order to lessen vessel damage.

Exchanging the soft 0.018 wire with a Pilot 50 wire retrogradely and another Pilot 50 wire antegradely, the kissing wire technique was accomplished to reach the main Pop a. Antegrade wire manipulation redirected the wire into Pronealis, A good achievement!!
 
Predilation was done using a 4-100 0.035 OTW balloon first, upsized to 6-120 0.035 OTW balloon for Pop a only. The result was good with dissections. So we decided to put stents at the ostium of ATA and PA and Pop a. The stents was coronary DES for ATA and PA with V stenting strategy and FKBP. Thereafter 2 Self expanding stents was deployed for SFA-Pop a. with good result
 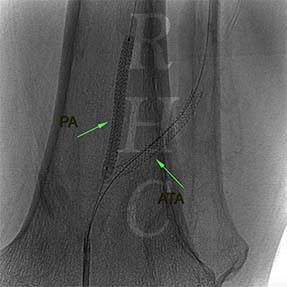
Here you can see the deployment of Pop Stent and the final result
 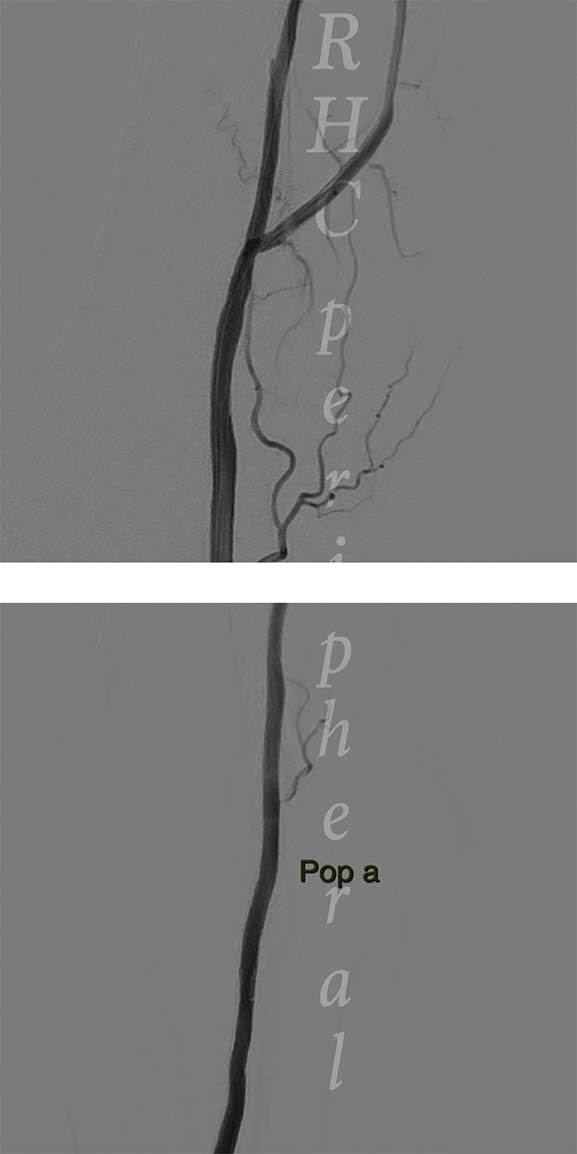
The final step is to evaluate the distal flow. As the retrograde approach may damage the last remained vessel this final step is very important. The angiogram showed a good distal flow and small oozing of blood at the site of retrograde access.

در پایان پروسیجر نبض دیستال ایجاد و پای بیمار گرمتر شده بود. در نهایت برای بیمار پانسمان هیدروژل بر روی زخم تعبیه شد. بیمار بدون عارضه مرخص شده
اوپراتورها
دکتر امید شافع
دکتر سید جمال موسوی
|








 انتخاب وب سایت مورد نظر :
انتخاب وب سایت مورد نظر : 




